



The price of prescription drugs in the U.S. continues to be a concerning issue to the public, with KFF polling consistently showing the public supports various approaches to lowering prescription drug costs. Efforts to rein in drug costs have long been a priority for both federal and state policymakers. The Trump administration has recently taken steps to address drug costs through Executive Orders and multiple pricing agreements to bring ‘Most Favored Nation’ pricing to consumers in the U.S., though the impact and savings from these efforts are not yet known. The Biden administration enacted the Inflation Reduction Act of 2022, which authorized the federal government to negotiate lower drug prices with manufacturers for some drugs covered by Medicare, among other provisions, resulting in an estimated reduction in the federal deficit of $237 billion over 10 years for the drug pricing provisions alone.
One player in the system of pharmaceutical pricing in the U.S. that has come under increasing scrutiny in recent years is the pharmacy benefit manager, or PBM. These so-called ‘middlemen’ are used by health insurance companies to manage their pharmacy benefits. PBMs have been the focus of attention from policymakers for several reasons, including their business practices, market consolidation, and lack of transparency, all of which factor into concerns that PBMs themselves have played a role in increasing drug prices, even as they work to manage pharmacy benefits and costs for insurers.
In an April 2025 Executive Order, the Trump administration directed the Assistant to the President for Domestic Policy to reevaluate the role of ‘middlemen’ to “promote a more competitive, efficient, transparent, and resilient pharmaceutical value chain”. In the current session of Congress, legislation addressing various concerns related to PBMs and their business practices has been introduced and voted on but not enacted, including provisions in recent House GOP legislation responding to the expiration of the enhanced ACA premium subsidies, which passed the House in December 2025, and in budget reconciliation legislation passed by the House but not the Senate in May 2025. This brief provides an overview of the role of PBMs in managing pharmacy benefits, discusses recent federal legislation focusing on several elements of PBM business practices, and explains the potential federal budgetary impact of this legislation, which would have a relatively modest impact on the federal deficit, based on available CBO estimates. (This brief focuses on actions at the federal level and does not address state legislative efforts related to PBMs, which have occurred in all 50 states.)
The Role of PBMs
Pharmacy benefit managers (PBMs) act as intermediaries between drug manufacturers and insurance companies that offer drug benefits to employer health plans, Medicare Part D prescription drug plans, state Medicaid programs, and other payers. In this role, PBMs serve several functions: negotiating rebates and price discounts with drug manufacturers, processing and adjudicating claims, reimbursing pharmacies for drugs dispensed to patients, structuring pharmacy networks, and designing drug benefit offerings, which includes developing formularies (lists of covered drugs), determining utilization management rules, and establishing cost-sharing requirements.
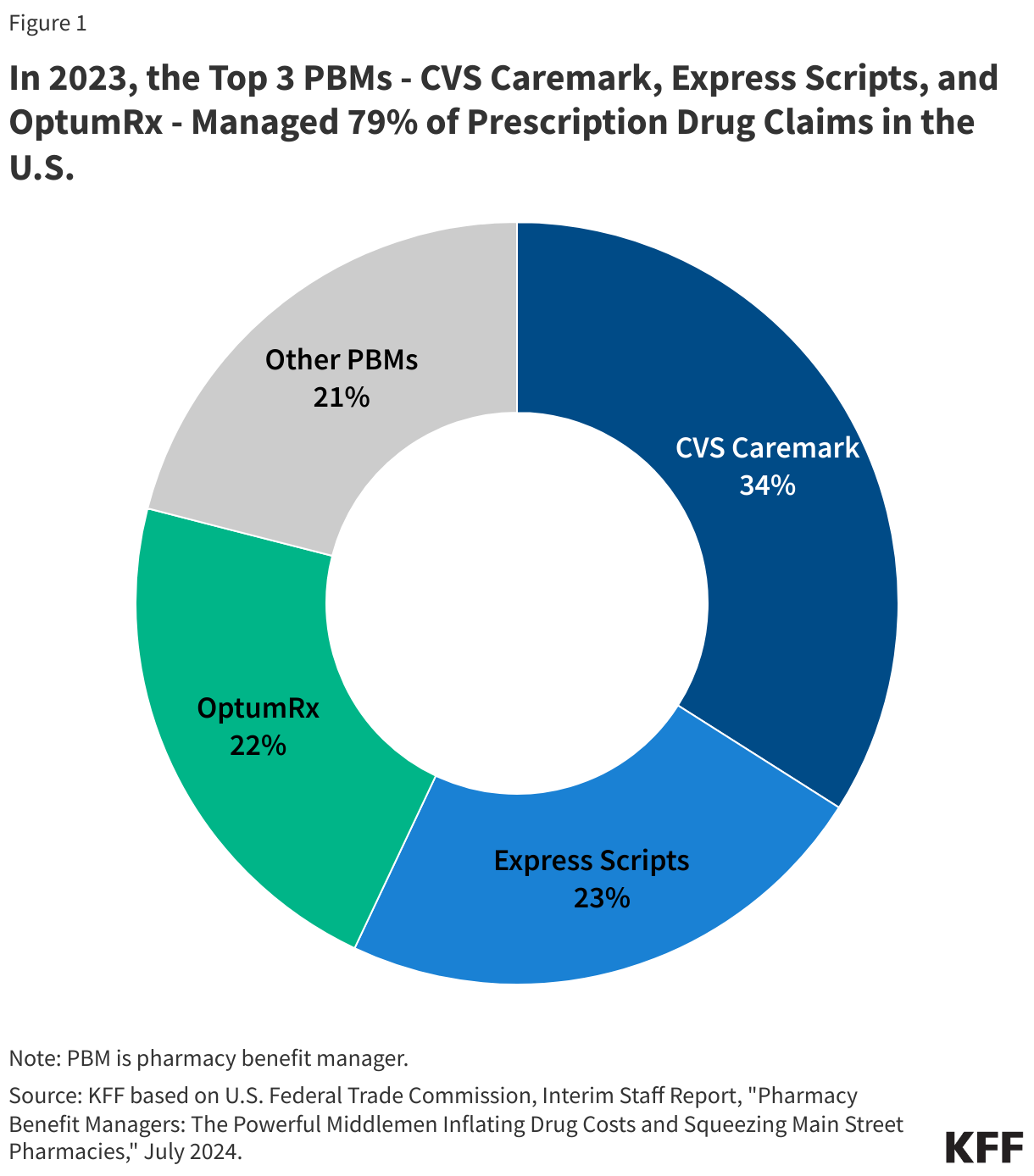
Although there are many PBMs, a few companies dominate the overall U.S. market. According to the Federal Trade Commission (FTC), the top 3 PBMs – OptumRx (owned by UnitedHealth Group), Express Scripts (owned by Cigna), and CVS Caremark (owned by CVS Health, which also owns Aetna) – manage 79% of prescription drug claims on behalf of 270 million people in 2023 (Figure 1).
Certain PBM Business Practices Have Given Rise to Concerns About Their Impact on Drug Prices
Sources of revenue: PBMs generate revenue in different ways. PBMs are typically paid fees for the functions they serve managing pharmacy benefits. PBMs also negotiate rebates with drug manufacturers in exchange for preferred placement of rebated drugs on a health insurance plan formulary, and they may retain a portion of the drug rebates they negotiate, though this may be more common in the commercial employer market than in the Medicare Part D market. Many state Medicaid programs and Medicaid managed care plans also contract with PBMs to manage or administer pharmacy benefits, including negotiating supplemental prescription drug rebates with manufacturers.
Rebates can help lower the cost of drug benefits for health insurers, which enables them to offer lower premiums in turn and may translate to lower out-of-pocket costs for patients at the point of sale. In order for PBMs to maximize rebate revenue, however, they may favor higher-priced drugs with higher rebates over lower-priced drugs with low or no rebates in their negotiations with drug companies. This may have an inflationary effect on drug pricing by manufacturers, increase costs for payers across the system, and raise out-of-pocket costs for patients who pay based on the list price – a particular concern for those without insurance but also for those with high-deductible insurance plans or when cost sharing is calculated as a percentage of the drug’s price, such as for Part B drugs under Medicare.
Because of these impacts, some have suggested that rebates negotiated between PBMs and drug manufacturers should be passed along in full to individuals at the point of sale and make discounts available upfront at the pharmacy counter. This arrangement would produce savings for individuals who take drugs with high rebates, since they would face lower out-of-pocket costs on their medications when they fill their prescriptions. However, if rebates are no longer being used to reduce a plan’s overall drug benefit costs, point-of-sale drug discounts could result in higher premiums for all plan enrollees.
Spread pricing: Another potential source of revenue for PBMs comes from the contracting practice of spread pricing, which is when a PBM pays a lower rate for a drug to the dispensing pharmacy than the amount the PBM charges an insurer for that drug and retains the difference or “spread” as profit. The practice of spread pricing can result in higher costs for insurers, while lower reimbursement levels put financial pressure on pharmacies.
PBMs have come under bipartisan scrutiny in recent years for spread pricing arrangements in Medicaid managed care that have increased Medicaid costs for states and the federal government. As a result, a number of states have prohibited spread pricing or adopted other reforms to increase transparency and improve oversight. Concerns about Medicaid spread pricing also led the Centers for Medicare & Medicaid Services (CMS) to issue an informational bulletin in May 2019 about how managed care plans should report spread pricing, which may have reduced the practice.
Consolidation: Consolidation in the PBM market has enabled a few PBMs to gain significant market power. As mentioned above, three PBMs manage nearly 80% of all prescription claims in the U.S. Moreover, the top three PBMs are vertically integrated with major health insurers: OptumRx is owned by UnitedHealth, Express Scripts is owned by Cigna, and CVS Caremark is owned by CVS Health, which also owns Aetna. Each of these PBMs also own mail order pharmacies and specialty pharmacies.
The FTC and members of Congress on both sides of the aisle have raised concerns that this level of market concentration and vertical integration enables PBMs to steer consumers to their preferred pharmacies, mark up the cost of drugs dispensed at their affiliated pharmacies, reimburse PBM-affiliated pharmacies at a higher rate than unaffiliated pharmacies for certain drugs, and apply pressure over certain contractual terms, all of which may disadvantage unaffiliated and independent pharmacies, contributing to pharmacy closures.
Transparency: Financial contracts between PBMs and drug manufacturers, including drug pricing information and the rebate arrangements that PBMs negotiate with drug manufacturers, are generally not made public. This means that plan sponsors often do not have insight into how much PBMs are actually paying for drugs on their formularies, and PBMs often consider this information to be proprietary. In the pharmaceutical supply chain as whole, many players operating in this market do not have information about prices, which can make informed decision-making difficult and imperfect.
In recent years, federal lawmakers have focused several Congressional hearings on the topic of PBMs, including their role in prescription drug pricing, drug spending growth, and rising out-of-pocket costs for drugs, and have introduced legislation focusing on several elements of PBM business practices. The legislation highlighted below is not an exhaustive list but includes some of the more recent and prominent legislative efforts in the 119th Congress.
In May 2025, the House passed a version of the 2025 federal budget reconciliation law that included several provisions that would have addressed some PBM operations, though the PBM provisions were not included in the final version of the bill that was passed by Congress and signed into law in July 2025 (sometimes referred to as the “One Big Beautiful Bill Act”). The provisions in the May 2025 House-passed budget reconciliation bill include:
- Delinking PBM compensation from drug prices, rebates, and discounts that they negotiate for drug plans under Medicare Part Dand instead basing compensation on a ‘bona fide service fee’, which would be a flat dollar amount.
- Establishing transparency and reporting requirements for PBMs, including data on utilization, pricing, and revenues for formulary covered drugs; PBM-affiliated pharmacies; contracts with drug manufacturers; and other PBM business practices. This provision would require PBMs to provide this data to Part D plan sponsors as well as the HHS Secretary.
- Prohibiting spread pricing in Medicaid and instead basing payments on a ‘pass-through model’ in which payments made by a PBM on behalf of the State Medicaid program to the pharmacy are limited to the drug ingredient cost and a professional dispensing fee. Payments to PBMs and similar entities would be required to reflect the pharmacies’ costs and an administrative fee that is fair market value.
- Ensuring accurate payments to pharmacies under Medicaid: All retail pharmacies and certain non-retail pharmacies would be required to complete the National Average Drug Acquisition Cost (NADAC) survey, if they are selected for participation in the survey. This provision would require survey participation across all retail pharmacies, including larger chain pharmacies who have historically not participated in the survey and who likely obtain their drugs at lower prices, which could lower pharmacy reimbursement for some drugs and result in federal and state savings.
In December 2025, the House passed GOP legislation responding to the expiration of enhanced ACA premium subsidies, the Lower Health Care Premiums for All Americans Act (H.R. 6703), which included a separate PBM provision that would increase oversight of PBMs that provide services to employer group health plans through data transparency and reporting requirements. This provision would require PBMs to report detailed prescription drug utilization and spending data to plans, including gross and net spending, out-of-pocket spending, pharmacy reimbursement, and other details related to the plan’s pharmacy benefit.
Separately, reflecting the bipartisan support for legislation related to PBMs, Representatives Buddy Carter (R) and Vincente Gonzalez (D) introduced the PBM Reform Act of 2025 in the House, while the chairman and ranking member of the Senate Finance Committee, Senators Mike Crapo (R) and Ron Wyden (D), introduced the Pharmacy Benefit Manager (PBM) Price Transparency and Accountability Act in the Senate. These bills are similar but not the same; the PBM Reform Act of 2025 includes the provision that would increase oversight of PBMs that work with employer group health plans (as in the broader House GOP bill), which is not included in the PBM Price Transparency and Accountability Act. A bipartisan group of representatives, including Representatives Jake Auchincloss (D), Diana Harshbarger (R), and James Comer (R) also recently reintroduced the Pharmacists Fight Back Act, which includes two coordinated pieces of legislation that would regulate PBMs in certain federal health benefits programs.
- The PBM Reform Act of 2025 (H.R.4317) includes most of the PBM provisions that were included in a preliminary version of the budget reconciliation bill that passed the House in May 2025 and includes: delinking PBM compensation from the cost of medications for drug plans under Medicare Part D, prohibiting spread pricing in Medicaid, and ensuring accurate payments to pharmacies under Medicaid. In addition, the bill includes provisions to increase oversight of PBMs that work with employer group health plans and to assure pharmacy access and choice for Medicare beneficiaries, which were not included in the May 2025 House-passed bill.
- The provision to assure pharmacy access for Medicare beneficiaries would reinforce existing regulatory requirements that Part D plan sponsors contract with any willing pharmacy that meets their standard contract terms and conditions and have those conditions be ‘reasonable and relevant.’ These conditions would be defined and enforced according to standards determined by the Secretary of Health and Human Services (HHS).
- The PBM Price Transparency and Accountability Act (S.3345) also includes most of the PBM provisions that were included in the May 2025 House-passed bill and includes: delinking PBM compensation from the cost of medications for drug plans under Medicare Part D, prohibiting spread pricing in Medicaid, and ensuring accurate payments to pharmacies under Medicaid. Additionally, it includes the provision to assure pharmacy access and choice for Medicare beneficiaries, which was not included in the May 2025 House-passed bill.
- The Pharmacists Fight Back Act (H.R. 6609) and (H.R. 6610) would establish certain requirements with regard to PBMs in Medicare and Medicaid and in Federal Employee Health Benefits Plans, respectively. Plan sponsors (or PBMs acting on behalf of those sponsors) would be required to reimburse pharmacies for drugs based on pricing benchmarked to the National Average Drug Acquisition Cost (NADAC) and would be required to share a portion of rebates at the point of sale, with the remainder of the rebates being used to lower plan premiums. The legislation also prohibits PBMs from steering patients to PBM-affiliated pharmacies.
Budgetary Effects of PBM Legislation
In general, cost estimates from the Congressional Budget Office (CBO) have scored PBM provisions with relatively low savings to the federal government. CBO estimated a total federal deficit reduction of $3.2 billion over 10 years (2025-2034) attributable to the PBM provisions incorporated in the May 2025 House-passed budget reconciliation bill (which were not included in the final legislation enacted in July 2025):
- A reduction of $400 million from delinking PBM compensation from the cost of medications for drugs under Part D and establishing PBM transparency and reporting requirements
- A reduction of $261 million from prohibiting spread pricing in Medicaid
- A reduction of $2.5 billion from ensuring accurate payments to pharmacies under Medicaid
The provision to increase oversight of PBMs that work with employer group health plans was scored as part of the Lower Health Care Premiums for All Americans Act (H.R. 6703) that passed the House in December 2025. CBO estimated this provision would reduce the federal deficit by $1.9 billion over 10 years (2026-2035), with $1.8 billion in additional revenues and savings of $22 million. CBO assumes this provision would modestly reduce premiums charged in the group health insurance market, which could increase wages and therefore increase federal revenues.
CBO has not provided cost estimates for the PBM Reform Act of 2025, the PBM Price Transparency and Accountability Act, or the Pharmacists Fight Back Act. The provision to assure pharmacy access and choice for Medicare beneficiaries is not reflected in any of the cost estimates above. It is also possible that the effects of the Medicaid spending reductions in the budget reconciliation law will impact estimates of savings from the Medicaid PBM provisions. The law is expected to result in fewer Medicaid enrollees, which could lower Medicaid drug spending and translate to lower savings from Medicaid PBM provisions.



