


On December 18, 2025, the Centers for Medicare and Medicaid Services (CMS) issued two proposed rules that would further limit youth access to gender affirming care. One rule would change the hospital Conditions of Participation (CoPs) which would prohibit most Medicare and Medicaid enrolled hospitals from providing specified gender affirming medical care for youth (the proposed CoPs rule). The second proposed rule would prohibit federal Medicaid or CHIP funds from covering this care for youth (the proposed Medicaid rule). Despite gender affirming care being considered a best practice model of care and consisting of interventions recommended by major medical associations, if finalized and implemented, the proposed rules would have a sweeping impact, albeit for a small number of young people, significantly limiting their access to these services.
The rules broadly align with a range of other administrative actions that take a multipronged approach to restrict this care. In particular, the proposed rules follow a January 2025 Executive Order that set a pathway for limiting youth access to gender affirming care and directed the Secretary of Health and Human Services (HHS) to “take all appropriate actions to end” gender affirming care for youth, including in Medicaid, and which specifically identified the CoPs as a possible vehicle for this. Additionally, on April 11, 2025, CMS sent a State Medicaid Director’s letter with the stated purpose of “reminding states of their responsibility to ensure that Medicaid payments are consistent with quality of care and that covered services are provided in a manner consistent with the best interest of recipients” and appearing to encourage states to take steps to limit gender affirming care for youth within their state Medicaid programs. Then, in May 2025, HHS sent a second letter to an unspecified group of providers, state medical boards, and health risk managers urging them to update treatment protocol to move away from provision of gender affirming medical care.
The proposed rules do not take effect immediately. Both have a 60-day comment period following their publication in the federal register. Then, following the comment period, CMS is tasked with considering the comments and could ultimately choose to finalize the proposed rule—either in amended form or as currently written—or elect not to do so. If finalized, both rules will likely face legal challenges, which could further slow implementation.
The Proposed Conditions of Participation (CoPs) Rule
If finalized, the proposed hospital CoPs rule would limit gender affirming care for youth, regardless of payer. The CoPs rule proposes to prohibit certain hospitals (i.e. those covered by section 42 CFR part 482) that accept payments from the Medicare or Medicaid programs from providing identified pharmaceutical and surgical services related to gender affirming care to young people under age 18. Prohibited services would include puberty blockers (which delay the onset of puberty), hormone therapy, and surgery (which is very rare among youth). While these services would be prohibited for the purposes of providing gender affirming care, the rule would permit hospitals to provide them to youth in some scenarios when the service is not intended to affirm a person’s gender.
The changes under the proposed CoPs rule represent a condition based on facility type (not payer) and therefore, if adopted, would prohibit hospitals from offering gender affirming services to all patients under 18 years old, regardless of payer, including youth with private insurance or other coverage and those paying cash, not just those covered by Medicare and Medicaid. It does not prohibit other types of facilities (e.g. free standing clinics, primary care or specialist providers in other settings) from offering these services (there are a variety of CoPs for providers which are not affected by the proposed CoPs rule).
Hospital Conditions of Participation (CoPs) are currently used to regulate how services can be provided safely and with high quality, rather than prohibiting specific services from being offered altogether. There are a variety of CoPs across different provider types which set standards and requirements, primarily related to quality and safety of care that health care providers must generally meet to participate in and receive reimbursement from Medicare and Medicaid. Hospital CoPs regulate a variety of administrative functions and health care services, including a hospital’s responsibilities to its patients, obligations of the hospital’s governing body, requirements related to emergency preparedness and planning, staffing requirements, minimum medical record requirements, and processes to develop safety procedures and quality improvement plans. While the proposed rule states that it is offering the revision to existing hospital CoPs regulations to address “the health and safety of children,” there is no medical consensus that gender affirming care represents a safety issue, and using hospital CoPs this way marks a departure from their current function of regulating how services can be performed (e.g., by licensed professionals, with equipment like defibrillators available during surgeries, etc.), rather than which services can be provided.
Hospital compliance with the CoPs is monitored with detailed surveys conducted by state agencies or accredited organizations (like the Joint Commission on Accreditation of Hospitals). These surveys are conducted during onsite visits to the hospitals; CMS usually gives hospitals time to fix violations. When hospitals are unwilling or unable to fix violations, CMS issues a termination notice, which happens relatively rarely. Medicare and Medicaid do not reimburse services rendered at terminated hospitals.
If finalized, the rule would apply to most hospitals in the United States. The proposed rule estimates there are a total of “4,832 Medicare/Medicaid certified hospitals” (covered by section 42 CFR part 482) that would be subject to its provisions. The restrictions would also apply to gender affirming care clinics and other clinics if they operate as a part of a hospital, including at off-campus locations. In 2023, the American Hospital Association identified more than 6,000 hospitals nationwide and it is likely that the large majority of hospitals not covered in the proposed rule and not included in 42 CFR part 482 are facilities such as Critical Access Hospitals and Rural Emergency Hospitals which are small rural facilities that may be less likely to offer gender affirming care. Although the proposal would apply to the large majority of hospitals, it is not clear what share of hospitals currently offer gender affirming care services for youth and many systems have recently stopped offering such services and have cited growing concern about pressure from the federal government (e.g. Los Angeles Children’s cited the “complex and uncertain regulatory environment” and Children’s National the “escalating legal and regulatory risks,” among many other examples).
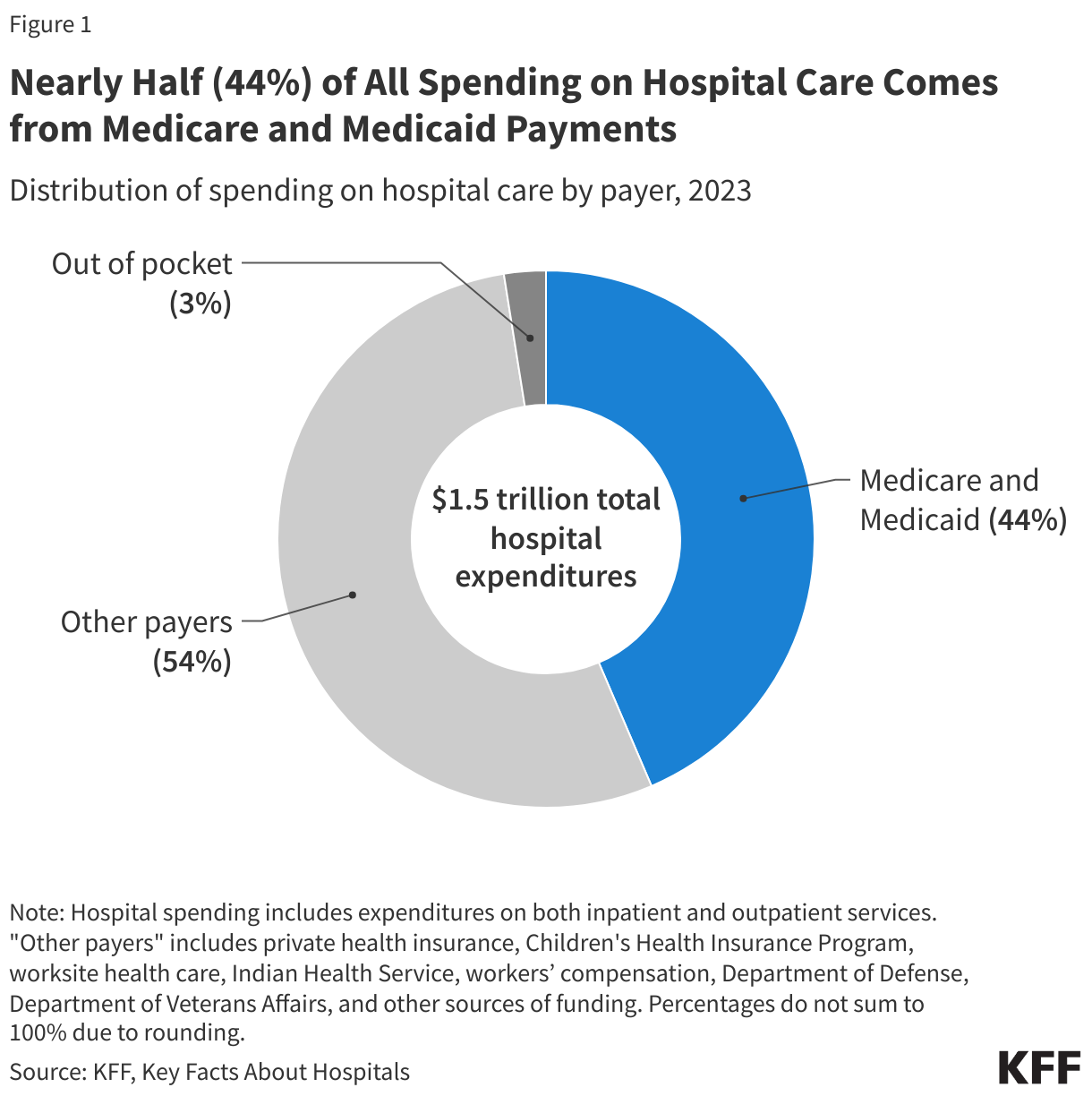
If the proposed CoPs rule were finalized, most hospitals would be prohibited from providing gender affirming care services for youth. Although hospitals could in theory stop participating in Medicare and Medicaid to continue providing gender affirming services, it is very unlikely that they would do so given the financial challenges this would present. Nationally, nearly half (44%) of all spending on hospital care comes from Medicare and Medicaid payments.
Although the rule would apply broadly to most hospitals, hospitals provide relatively few gender affirming care services and almost no gender affirming surgeries to youth. Accounting for states that already restrict youth access to gender affirming care, the proposed rule estimates the change would impact 8,570 young people. The Williams Institute estimates that there are approximately 724,000 trans identified youth (13-17) in the U.S. This suggests that approximately 1.2% of trans youth in the U.S. receive gender affirming medical services in hospitals and could be impacted by the proposal each year. As with past research, the CMS finds that most of this care is pharmacologic with surgery being very rare among transgender youth. The proposed rule identifies 85 surgeries in facilities that would be impacted by the rule over the course of one year nationwide. This represents less than 0.0003% of youth under 18 in the United States (based on the denominator of people aged 12 to 18 being 29,600,770 as described in the proposed rule).
Although gender affirming services could still be provided outside of hospitals subject to the proposed CoPs rule, there would be fewer facilities available in a landscape where accessing this care has already become challenging. Many types of gender affirming care sought by young trans people (such as puberty blockers and hormone therapies) can be provided in outpatient settings and therefore received at non-hospital providers. However, patients may need to travel farther and pay more to receive the set of services they need. They may also face challenges finding a specialized pediatric gender clinic offering a cross-specialty integrated care experience as those clinics are often based in hospital settings. Indeed, the proposal states young people may face “difficulty in identifying in-network providers that have available space and longer commute times to these providers” and assumes that 4,285 youth (half of those estimated to be impacted by the proposed rule) would stop receiving care.
The Proposed Medicaid Rule
The proposed Medicaid rule would prohibit the use of federal Medicaid and CHIP funds to cover the specified gender-affirming care services, regardless of the site of care, limiting access for minors who are covered by these programs. The specified services are the same pharmaceutical and surgical services the CoPs proposed rule seeks to bar. Unlike the CoPs proposal, which seeks to limit access at the hospital level (regardless of coverage type), the Medicaid proposal seeks to limit funding for services for youth based on their coverage source (i.e. Medicaid or CHIP) and would therefore restrict reimbursement for care regardless of provider type (e.g. hospitals, primary care providers, endocrinologists, etc.). However, it does not prohibit providers from offering these services. Based on statutory definitions of “minor” the proposed rule would prohibit federal Medicaid reimbursement for this care to those under 18 years of age, while separately administered CHIP programs would limit reimbursement for people through age 18. (CMS is requesting comment on the feasibility of implementing the proposal with these age differences in Medicaid compared to CHIP.) As with the CoPs proposed rule, although Medicaid programs would be prohibited from covering the identified services for gender affirming care with federal funds, programs would be permitted to reimburse for these same services for youth when used for other purposes. Also, similar to the CoPs proposed rule, these health programs could cover other related services such as psychotherapy, which is a common part of gender affirming care services, especially for youth.
Although the proposed rule would prohibit states from using federal Medicaid or CHIP funds to cover gender affirming care, it would not restrict states from covering these services using state-only dollars. It is likely that different states will make different choices about whether or not to cover these services using state funds. Already, some states restrict coverage of gender affirming care in their Medicaid and CHIP programs.
The Medicaid proposed rule (unlike the CoPs proposal) does not offer an estimate on the number of individuals it would impact but it does find that only a very small share of Medicaid/CHIP funds are spent on gender affirming care, likely suggesting low utilization. Although the impact of the proposed Medicaid restrictions would be meaningful for individuals and families, only a very small amount of Medicaid funding is spent on services for which the Medicaid proposed rule would prohibit reimbursement. In the proposed rule, CMS estimates that Medicaid spent about $31 million on the specified services for enrollees aged 18 years and younger in 2023. This represents about 0.003% of all Medicaid spending that year (based on the proposed rule’s spending estimate and FY 2023 total Medicaid spending). Of this total ($31m), CMS finds most of the spending occurred on services provided to older teens, with two-thirds of identified spending (66%) occurring among those 15-18 years old. Notably, this includes some spending for 18-year-olds, some of whom would not be impacted by the proposal. Nonetheless, the agency’s analysis supports the conclusion of other researchers that utilization of gender affirming medical services is relatively rare among adolescents and most spending is nonsurgical. Ninety-two percent (92%) of spending on the specified services for enrollees aged 18 years and younger was nonsurgical and almost all surgical spending (98%) occurred among youth in the 15-18 age group. It is not possible to know how much of this was spent on eighteen-year-olds, a group not impacted by this policy, and the age of majority in most states.
KFF estimates 37% of people under 18 in the United States are covered by Medicaid or CHIP with variation across states. Applying state specific shares of youth enrolled in Medicaid to Williams Institute state level estimates of trans youth (and assuming the coverage distribution among trans youth is similar to youth in general), KFF estimates there to be approximately 270,000 trans youth covered by Medicaid or CHIP. We estimate that, approximately, 138,000 young trans people with Medicaid or CHIP live in a state without a state law prohibiting gender affirming care (and without a state-based Medicaid ban) and could face insurance limitations under the proposed Medicaid rule, if they sought gender affirming care. Notably, not all transgender youth would seek or desire access to the proposed restricted services, and the CoPs rule, along with other research, finds uptake of gender affirming medical services is low. Nonetheless, if finalized, the proposed rule could foreclose on their ability to receive covered care.
While young people with Medicaid and CHIP coverage could theoretically seek care outside of hospitals without using their insurance, the cost of doing so would likely be prohibitive. Families with children covered by Medicaid and CHIP have low to moderate incomes and would face difficulty paying for any uncovered care.
Looking Ahead
As noted earlier, the proposed rules do not take effect immediately. If finalized (following a 60-day comment period), these proposed rules taken together would lead to youth access to gender affirming care being further limited. Patients with the most financial and other supportive resources would have the greatest ability to navigate access (e.g., travel long distances to providers offering these services or have commercial insurance which might cover gender affirming care), whereas those with more limited resources and Medicaid/CHIP coverage, which is by definition insurance for low-income families, could find accessing services the most challenging. The rules would not limit other care for transgender young people.
Losing access to gender affirming care could have meaningful health implications for young people and their families. Research has demonstrated that young transgender people’s mental health is negatively impacted when this care is denied, including leading to an increased risk of suicidality and that when care is received, well-being is improved. Hospitals with larger gender affirming care programs may also be conducting academic or clinical research on the experiences of and care for young transgender patients. If these hospitals close or limit their services, that may change or eliminate their ability to do this research.
Immediately following their release, the proposals faced criticism from the American Academy of Pediatrics which wrote, “these rules are a baseless intrusion into the patient-physician relationship” and that the association “remains committed to ensuring that all children — including gender-diverse youth and children covered by Medicaid — receive care that is backed by science, delivered with compassion, and offered without political interference.”
There has been significant litigation challenging efforts to limit gender affirming care at both the state and federal level and if finalized, lawsuits challenging these rules would be likely and could happen on multiple grounds (e.g., Constitutional, Administrative Procedure Act (APA), Section 1557 of the Affordable Care Act (ACA), and violations of Medicaid and Medicare statute and/or regulations, etc.). Indeed, the ACLU has already suggested a willingness to challenge these are regulations, stating that “if this administration moves forward with this attempt to enact a national ban on our medical care through coercion, the ACLU will see them in court.” Additionally, multiple state attorneys’ general have stated that they oppose the rule and plan to fight its implementation.



