



On December 29, 2025, the Centers for Medicare & Medicaid Services (CMS) announced first-year state awards from the $50 billion Rural Health Transformation Program (the “rural health fund”), which is being administered by a new Office of Rural Health Transformation. The rural health fund was created as part of the July 2025 budget reconciliation law, sometimes called the One Big Beautiful Bill, to help offset the impact on rural areas of the law—which includes an estimated $911 billion in federal Medicaid spending reductions over ten years, including an estimated $137 billion in rural areas. All 50 states applied for the rural health fund, and each state received an award. CMS will distribute $10 billion each year from fiscal years 2026 through 2030, beginning this year.
State awards for 2026, the first of five years, average $200 million, ranging from $147 million in New Jersey to $281 million in Texas (Figure 1). Differences in total awards across states in the first year (and most likely in future years) are modest relative to large differences in rural populations and rural health needs more generally. For example, Texas has about thirty times as many rural residents as New Jersey (4.3 million versus about 140,000) but is only receiving about twice as much funding in the first year ($281 million versus $147 million). Differences in total awards across states are relatively modest primarily because half of the rural health fund (50%) is being distributed equally across approved states, regardless of need, as required by law. Because all states have been approved for funding, each is slated to receive $100 million from this half of the fund in 2026 and in each year from 2027 through 2030.
Texas, Alaska and California are receiving the largest total awards in the first year. While Texas and California have the largest and fourth-largest rural populations in the country, respectively, Alaska has the fifth smallest rural population. Alaska likely received a relatively large award at least in part because a portion of the fund was distributed to the five largest states based on land area. New Jersey, Connecticut, and Rhode Island are receiving the smallest awards in the first year. These are all states with relatively small rural populations.
Figure 1
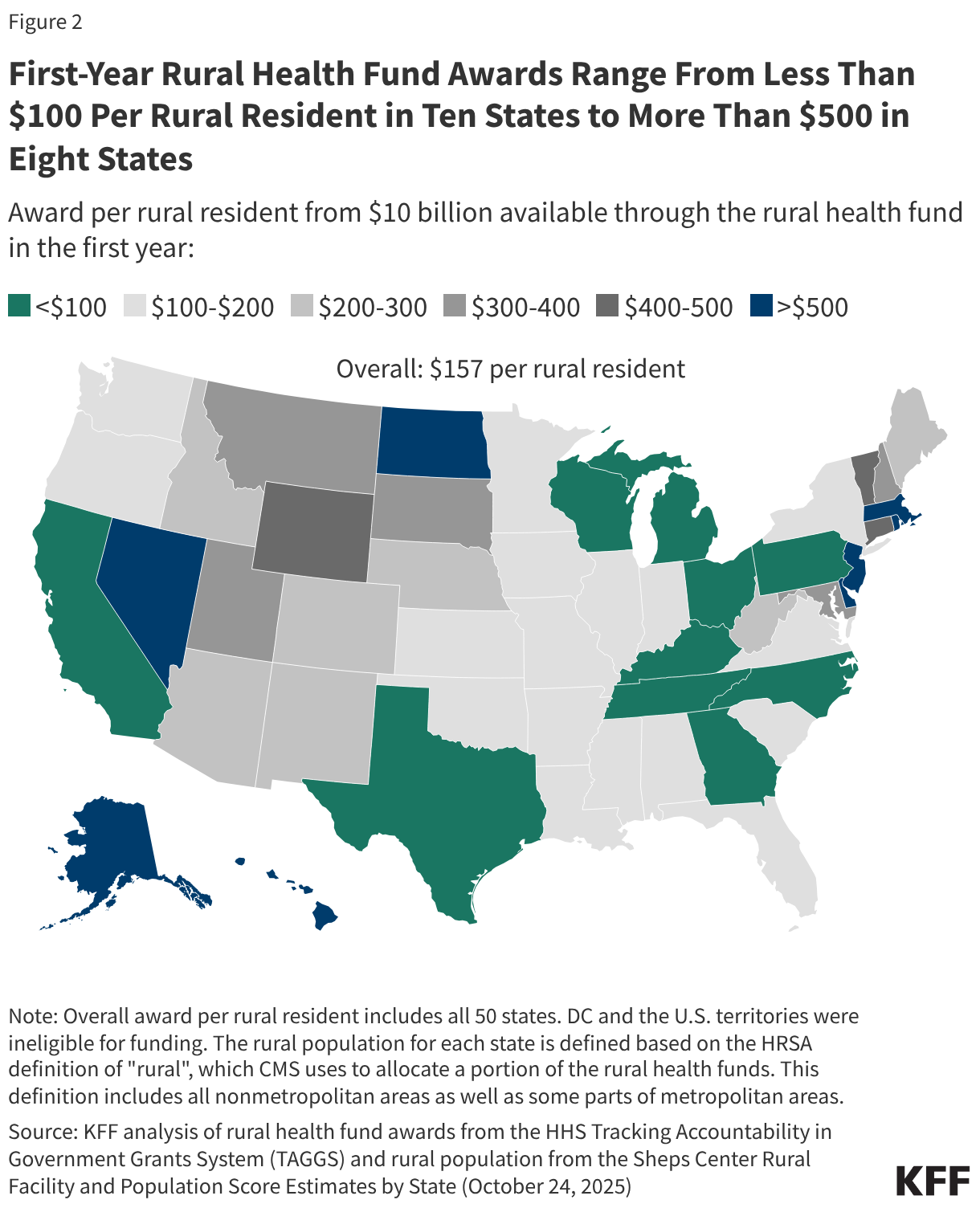
First-year awards per rural resident vary widely across states, ranging from less than $100 in ten states to more than $500 in eight states according to KFF analysis (see Figure 2). State awards are partially, but not closely, tied to rural population, meaning that first-year awards per rural resident are generally relatively small among states with the largest rural populations. For example, Texas has the largest rural population in the country—and the largest total award in the first year—but will receive the smallest payment per rural resident ($66 in 2026). In contrast, states like Rhode Island, New Jersey, and Alaska, with far fewer rural residents, will receive substantially higher amounts per rural resident ($6,305, $1,069, and $990 respectively, with Rhode Island being an extreme outlier). Only a quarter of the $50 billion fund is being distributed exclusively based on measures of state need, with just 5% of the fund that is based on rural population. Other measures of need, according to CMS, include the number of rural facilities, land area, the share of hospitals receiving Medicaid disproportionate share hospital (DSH) payments, and other factors.
While lawmakers created the fund in part to help offset the impact on rural hospitals of cuts under the reconciliation law, CMS has made clear that funding is intended to benefit rural communities more broadly by transforming health care systems. Examples of state initiatives based on the subset of state applications available to the public and abstracts posted on CMS’s website include initiatives related to Make America Healthy Again (MAHA) (such as improving access to healthy foods and preventing and managing chronic conditions), expanding telehealth services and remote patient monitoring, rural workforce development programs, and supporting regional collaboration among providers.
CMS stipulates that payments to hospitals and others for patient care cannot exceed 15% of total funds, though providers could benefit in other ways, such as through investments in existing buildings and infrastructure (restricted to 20% of total funds). It is unclear how much of the money will benefit rural hospitals either directly or indirectly and the extent to which this will offset hospitals’ losses under the reconciliation bill. Moreover, it is not yet clear how much information will be available to the public to track the flow of dollars from states to rural providers and other entities and to evaluate the effectiveness of state initiatives.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.



