As widely expected, and following a recent Presidential memorandum, the Department of Health and Human Services (HHS) issued a memo on January 5, 2026 implementing major changes to the government’s recommended vaccination schedule for children, adding to other changes previously made in 2025. Collectively, these changes reduce the number of vaccines recommended for all children and, as such, have important implications for childhood immunizations and U.S. public health broadly, especially given the context of already declining childhood vaccination rates and ongoing outbreaks of diseases such as influenza and measles. While states, not the federal government, ultimately determine which vaccines are recommended for children and required for school entry, the federal government has significant influence over vaccine policy and access. This policy brief provides an overview and identifies several implications of these changes.
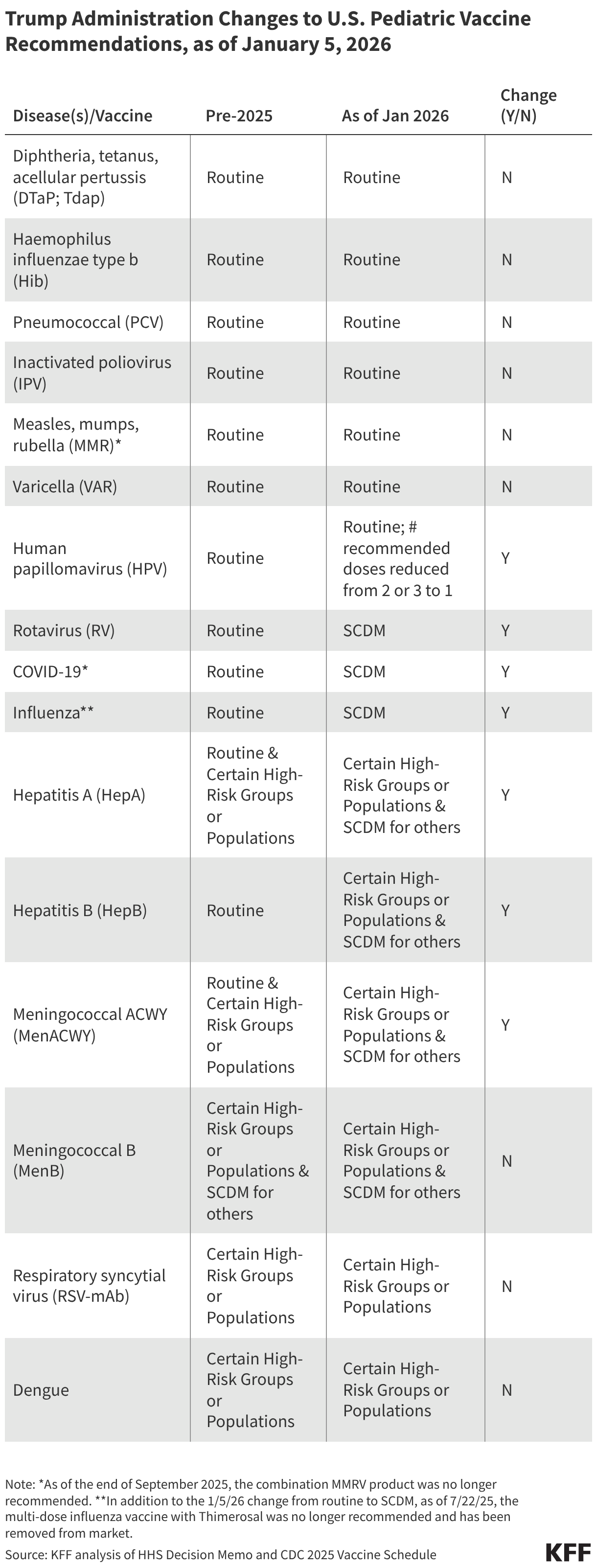
Starting in 2025, changes by HHS to routine vaccine recommendations for children have reduced the number of diseases targeted from 17 to 11 and the number of routine vaccines from 13 to 7 (see Table). Due to changes starting in October of last year, there are now six vaccines no longer recommended for routine use by all children in the United States: rotavirus, COVID-19, influenza, hepatitis A, hepatitis B, and meningococcal vaccines. Instead, some of these vaccines are now recommended for a narrower group of children, based on certain risk criteria or other specific factors, and all six have been moved from the routine category of vaccination to “shared clinical decision making,” a process that is “individually based and informed by a decision process between the health care provider and the patient or parent/guardian.” Beyond these changes, while HPV vaccine remains routinely recommended, HHS has reduced the number of recommended doses from two or three (depending on age of initial vaccination) to one.
Insurance coverage for childhood vaccines is not expected to change, although there is one exception. Most insurers are required to cover ACIP/CDC recommended vaccines at no-cost (including those recommended through SCDM), either due to requirements of the Affordable Care Act or other federal statutes and as such, these changes should not affect coverage, as also stated by HHS officials. Thus, parents wishing to vaccinate their children against diseases no longer recommended for all children but available through SCDM may still do so without having to be concerned about out- of-pocket costs. One potential exception relates to the HPV vaccine: now that the federal government recommends just one dose of HPV (instead of the previously recommended two to three doses), insurers will not be required to cover an additional dose should parents seek one (the current commercial price for one dose is more than $300). Through the end of 2026, however, health insurers have pledged to continue to cover all vaccines that were recommended in the prior childhood vaccine schedule and several states have moved to mandate free coverage by state-regulated insurers, and could choose to include additional doses.
The new schedule positions the U.S. as an outlier among peer nations in routinely recommending so few vaccines for children. One of the main reasons cited for the new schedule was that the U.S. was an outlier compared to peer countries in recommending so many routine vaccinations for children. Denmark was cited, both at a recent federal advisory committee meeting and in the HHS decision memo, as a model for the U.S. to emulate. The changes made now closely align the U.S. with Denmark (with the only difference being the varicella vaccine which is recommended by the U.S. but not Denmark). No other country among the 20 peer nations that HHS compares the U.S. to in its decision memo recommends vaccines against as few diseases as Denmark, which makes that country, and now the U.S. also, an outlier in this group. For comparison, Australia, Austria, Germany, Greece, Ireland, Italy, Japan, New Zealand, Spain, and the United Kingdom all recommend vaccinating children against 14 or more diseases. More broadly, each country has its own process and unique set of circumstances when it comes to determining vaccine recommendations, and each has developed their childhood vaccination schedule after years of reviewing and weighing available evidence in light of many factors, such as differences in health delivery systems, insurance coverage, public health system capacity, and national priorities. To date no high-income country has made its vaccination decisions based only on what a “peer” country does.
The process used to make these changes marks a departure from the past and further changes are signaled ahead. Historically, any major changes to federal vaccine recommendations were developed through an established, deliberative process that included internal government review with experts from the Center for Disease Control and Prevention (CDC) and other agencies, as well as consideration and public debate via meetings of the Advisory Committee of Immunization Practices (ACIP), the external expert advisory group to CDC. Recent changes made under HHS Secretary Kennedy, however, have circumvented this process, and instead changes have been announced without much internal or external consultation, and without prior public notice. This occurred with Secretary Kennedy’s announcement on social media that HHS was narrowing its COVID-19 recommendations, and now with an announcement of a new childhood vaccine schedule that was not reviewed by CDC experts nor given a public hearing through ACIP. The White House and HHS have also stated they are examining other aspects of vaccine policy including examining whether the measles, mumps, rubella combination vaccine should be divided into separate shots, how vaccines are tested and safety is monitored, and whether liability protections for manufacturers should be reexamined, which could mean further changes to policy may be forthcoming without a standard review processes.
While HHS cites decreased vaccine uptake and declining trust as additional reasons for changing pediatric vaccine recommendations, it is unclear if these changes will address these issues and they could have the opposite effect. By narrowing the groups recommended to receive certain vaccines, the federal government’s changes could lead parents and providers to choose to vaccinate less often than they have previously. Taking a cue from the new federal vaccine schedule, some states may also loosen vaccine requirements for school attendance, which could also result in lower vaccination coverage. In addition, moving vaccines from a routine, universal recommendation to a shared clinical decision-making (SCDM) recommendation can add an additional step or introduce other barriers to vaccine access, further depressing vaccination rates. With six vaccines newly placed in the SCDM category, such barriers could lead to more missed opportunities for vaccinations. In addition, even though federal health officials state that the new schedule is designed to create more public trust in vaccines, it’s not clear how it may affect trust and it could very well do the opposite. Most parents in the U.S. do not believe there are too many recommended vaccines, though MAGA Republican and MAHA parents – a minority of parents overall – are more likely to agree that the government should recommend fewer vaccines. Many states and expert groups are already making vaccine recommendations that differ from those of the federal government, and the new schedule is likely to exacerbate the conflicting messages that parents and providers hear about vaccines. For now, parents and providers will have to navigate a landscape of conflicting messages and recommendations about vaccines, which sows confusion and ultimately makes it harder for people to know what to do.
There will be differential impacts of these changes across the country. Ultimately, it is state and local jurisdictions that hold primary responsibility for determining key childhood vaccine policies, including which vaccines are recommended for routine use and which are required for school attendance. In light of changing federal guidelines that in many cases have narrowed vaccine recommendations, manystates have taken steps to de-link state policies and recommendations from those coming from the federal government, particularly Democratic-led states. For example, KFF analysis finds that 24 states no longer use HHS/CDC as a source for vaccine recommendations (up from just 13 in September 2025) and instead turn to state level or external expert groups such as AAP for guidance; a smaller number mandate free insurance coverage by state-regulated insurers for their own set of recommended vaccines. The divergence between federal policy and the states is likely to grow after the latest changes to federal recommendations, which means vaccine coverage and access could increasingly vary according to where one lives. More limited access in some states could, in turn, lead to decreased vaccine coverage and increased incidence of vaccine preventable diseases.
Tracking how the new vaccine schedule impacts vaccination rates in the U.S. may be challenging due to other HHS policies. It remains to be seen how these new recommendations play out in terms of vaccination rates, but recent Trump administration policies may make tracking these changes more challenging. For example, CDC and other federal staffing and funding going to state and local public health efforts across the U.S. has been cut, jeopardizing data collection and analysis. Further, the Trump administration in December announced that, starting in 2026, states will no longer be required to report several measures related to immunization status to HHS as part of their Medicaid and CHIP reporting requirements. Given that nearly four in 10 children in the U.S. are covered by Medicaid, visibility on their vaccine status will be reduced going forward.