Many older adults and people with disabilities require assistance with self-care such as bathing, dressing, and eating. Help with such services is known as “long-term care” and may be provided in institutional settings such as nursing facilities or in people’s homes and the community, including assisted living facilities. Four-in-ten adults incorrectly believe that Medicare is the primary source of coverage for low-income people who need nursing or home care, but Medicaid is the primary payer—covering nearly two-thirds of all home care spending in the United States in 2023.
The 2025 reconciliation law is estimated to reduce federal Medicaid spending by $911 billion (roughly 14%) over a decade and may have broad implications for home care, including for the workforce, support for family caregivers, and states’ coverage of services. Over half of Medicaid spending finances care for people ages 65 and older and those with disabilities, the enrollees most likely to use home care and related services, and reductions of this magnitude will leave states with difficult choices to raise new revenues or reduce Medicaid spending. The reconciliation law also established a new type of 1915(c) home care waiver for people who do not need an institutional level of care. Take-up of the new waivers is expected to be low given the cuts to federal Medicaid spending and requirements for states to demonstrate that new waivers will not increase the average amount of time that people wait for existing waiver services. This issue brief provides an overview of what Medicaid home care (also known as “home- and community-based services” or HCBS) is, who is covered, and what services were available in 2025. Over 5 million people receive Medicaid covered home care services annually.
This brief is one of several describing data from the 23rd KFF survey of officials administering Medicaid home care programs in all 50 states and the District of Columbia (hereafter referred to as a state), which states completed between April and July 2025. Other issue briefs from the survey describe the number of people on waiting lists for home care, how states manage home care spending, how home care programs support family caregivers, and payment rates for home care providers. The survey was sent to each state official responsible for overseeing home care benefits (including home health, personal care, and waiver services for specific populations such as people with physical disabilities). All states except Florida responded to the 2025 survey, but response rates for certain questions were lower. Where possible, KFF supplemented survey data with previously reported or publicly available data to provide information for the states that did not respond. Survey findings are reported by state and waiver target population, although states often offer multiple waivers for a given target population. States generally completed the survey prior to enactment of the reconciliation law. Key takeaways include:
- Nursing facility care is a required Medicaid benefit, but states can choose whether to provide most home care services. A key component of home care is personal care, which helps people who need assistance with self-care (such as bathing and dressing) and household activities (such as taking medications and preparing meals).
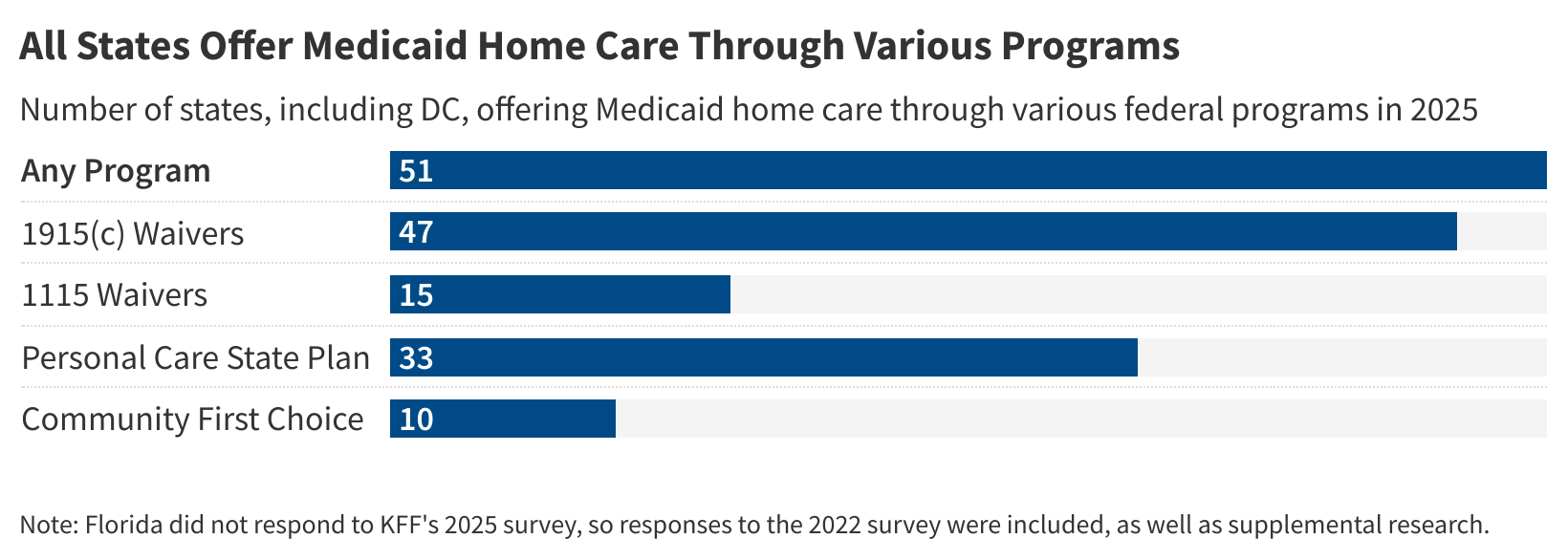
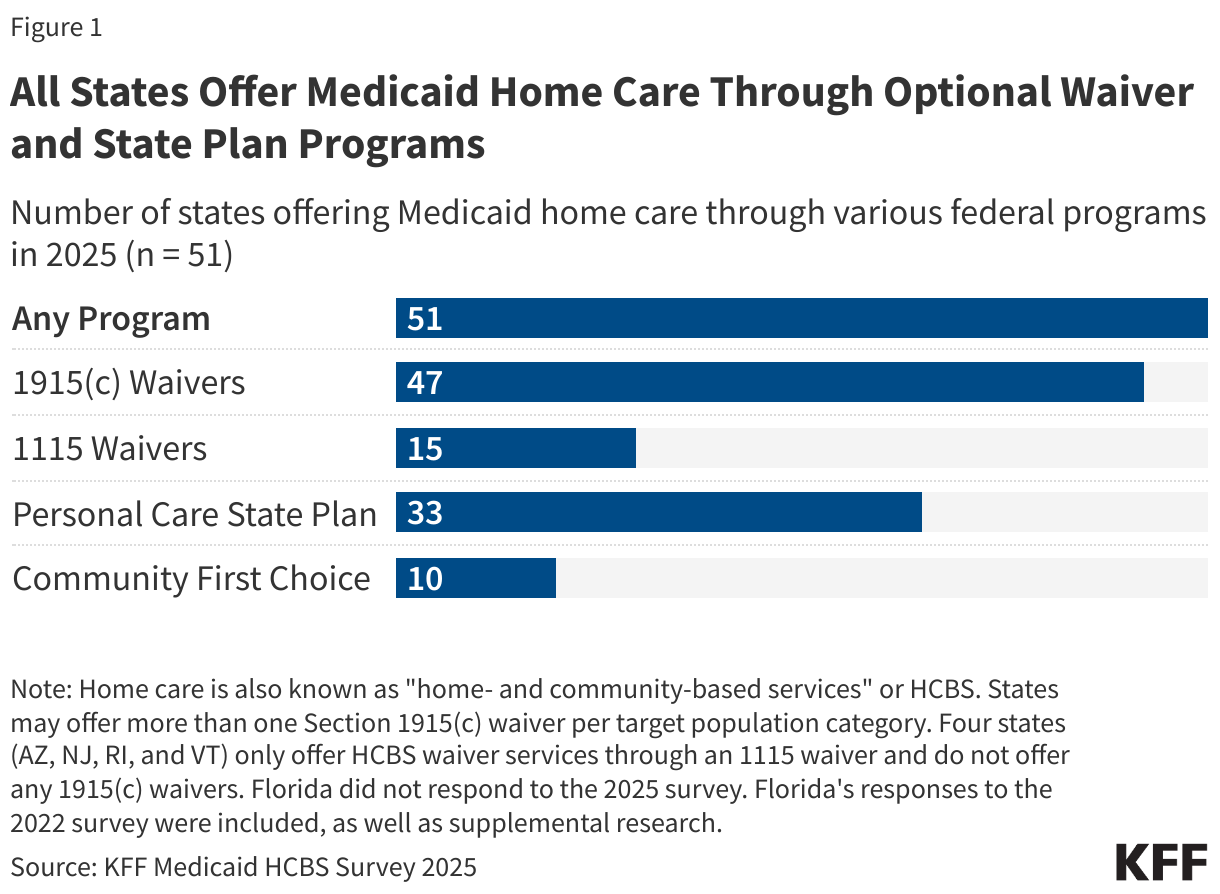
- Medicaid home care can be offered through either the Medicaid state plan or as part of a specialized waiver. All states offer Medicaid home care through waivers, most commonly 1915(c) waivers (47 states).
- Home care is also offered through 1115 waivers (15 states), personal care offered as a state plan benefit (33 states), or the Community First Choice option, which is also a state plan benefit (10 states, Figure 1).
- Most states provide Medicaid home care through waivers that offer benefits specifically targeted to people with intellectual or developmental disabilities (48) and people ages 65 and older or who have physical disabilities (46). For such waivers, most states offer multiple waivers for each population: Among states with intellectual or developmental disability waivers, only 16 offer one program, while 18 offer three or more; and among states with waivers serving people ages 65 and older or who have physical disabilities, 24 offer only one program and 10 offer three or more.
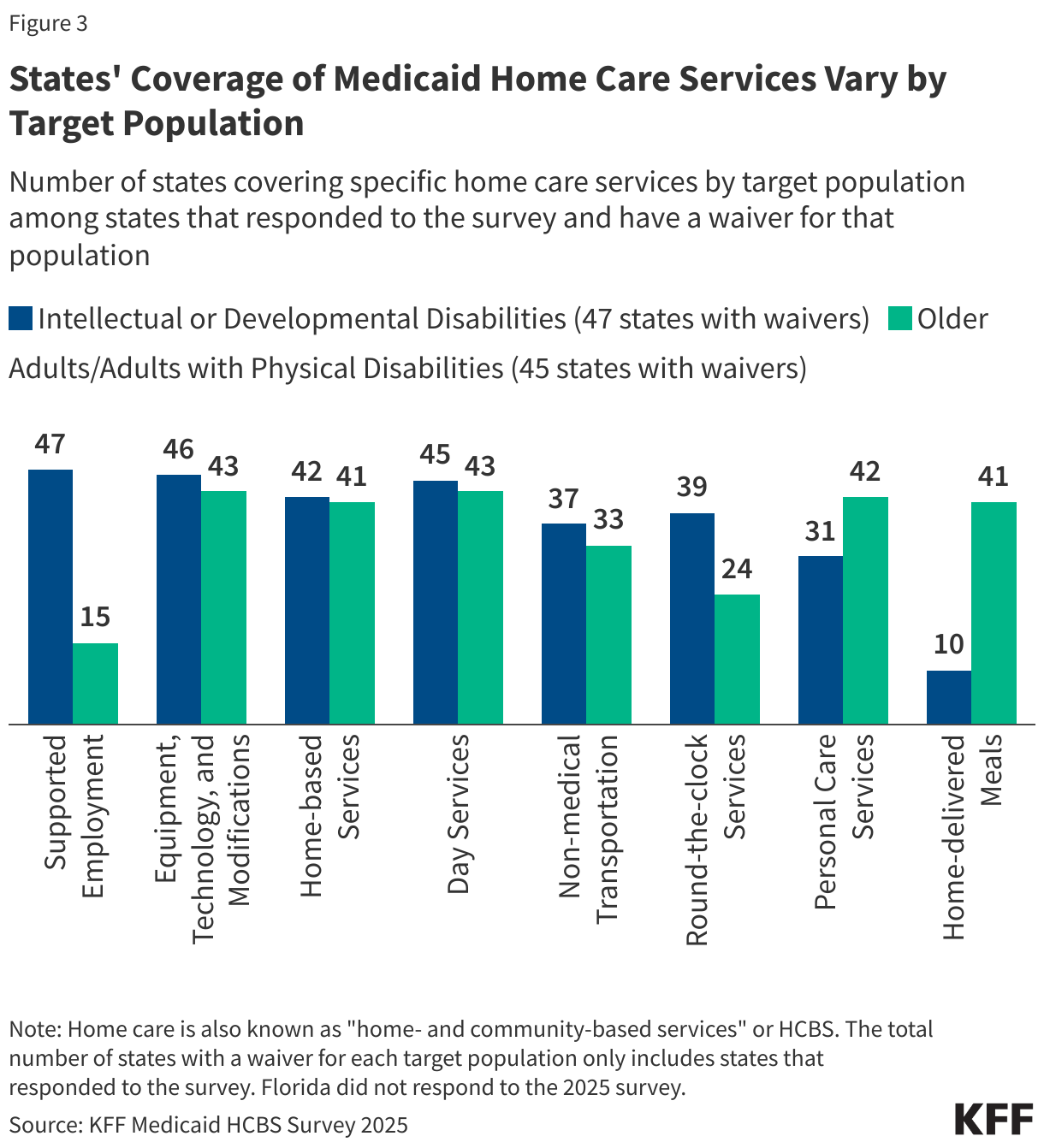
- Waivers’ coverage of different home care services, such as day services, supported employment, and home-based services, vary by the target populations they serve.
What programs do states use to provide Medicaid home care?
Unlike institutional long-term care, nearly all home care is optional for states to provide under Medicaid. States are required to offer cover home health—which consists of part-time nursing services; home health aide services; and medical supplies, equipment, and appliances suitable for use in the home—but all other home care services are provided at the discretion of the states. States use various federal legal “authorities,” also known as programs, to offer home care, which are generally categorized as being part of the Medicaid state plan or part of a waiver. If services are provided through a state plan, they must be offered to all eligible individuals. In contrast, services provided under waivers, such as 1115s or 1915(c)s, may be restricted to specific groups based on geographic region, income, or type of disability. Waivers may include a wider range of service types than can be provided under state plans, but states may limit the number of people receiving waiver services. When the number of people seeking services exceeds the number of waiver slots available, states may use waiting lists to manage participation in the waiver.
All states have at least one home care program and many states have multiple programs. Home care is most frequently offered through 1915(c) waivers (47 states) and the personal care state plan benefit (33 states), and less frequently offered through 1115 waivers (15 states) or the Community First Choice option (10 states, Figure 1). KFF estimates that 5.1 million people used Medicaid home care in 2023 compared with only 1.4 million people who used institutional long-term care.
All states offer people assistance with self-care and household activities under the personal care benefit, but they use different programs to do so. The primary home care benefit is personal care, which provides people with assistance with the activities of daily living (such as eating and dressing) and the instrumental activities of daily living (such as preparing meals and managing medication). States most commonly cover personal care through waivers (48 states), followed by the state plan (33 states).
How are people eligible for Medicaid home care?
Most people who are eligible for Medicaid home care qualify on the basis of having a disability or being ages 65 and older. Medicaid eligibility pathways in which eligibility is based on old age or disability are known as “non-MAGI” pathways because they do not use the Modified Adjusted Gross Income (MAGI) financial methodology that applies to children, pregnant individuals, parents, and other non-elderly adults with low incomes. In addition to considering income and age or disability status, non-MAGI eligibility pathways usually require people to demonstrate that they have limited savings and other financial resources (e.g., assets). Because nearly all non-MAGI pathways are optional, eligibility levels vary substantially across states.
Most states allow people with somewhat higher incomes to qualify for Medicaid home care, but income is capped at 300% of the supplemental security income limit ($2,901 per month in 2025) and assets are usually limited to $2,000 per person. Medicaid enrollees who use long-term care must also meet requirements related to their functional needs which are generally measured in terms of the ability to perform activities of daily living such as eating and bathing. Over half of people who use Medicaid home care are also enrolled in Medicare; such people are also known as dual-eligible individuals
In 2025, states operated over 300 different programs for Medicaid home care, many of which targeted a specific population. Most programs (259) were operated through 1915(c) waivers with 15 operated through 1115 waivers. The most common waiver programs target people with intellectual or developmental disabilities (48 states) and people who are ages 65 and older or have physical disabilities (46 states). States are likely to offer multiple waiver programs for the most common target populations, but states with less common waivers, such as those serving people with traumatic brain or spinal cord injuries or mental health conditions, typically only offer one program per target population.
Each year, some states’ waiver programs change, but in general, the trend has been towards offering more waivers. In 2025, only one state, Oregon, had new waivers and no states eliminated waivers. In Oregon, there is a new 1115 waiver for people who are ages 65 and older or have physical disabilities that provides in-home support services and support for family caregivers and a new 1915(c) waiver that allows parents of minor children with disabilities to be paid for providing attendant care to their child.

What services does Medicaid home care cover?
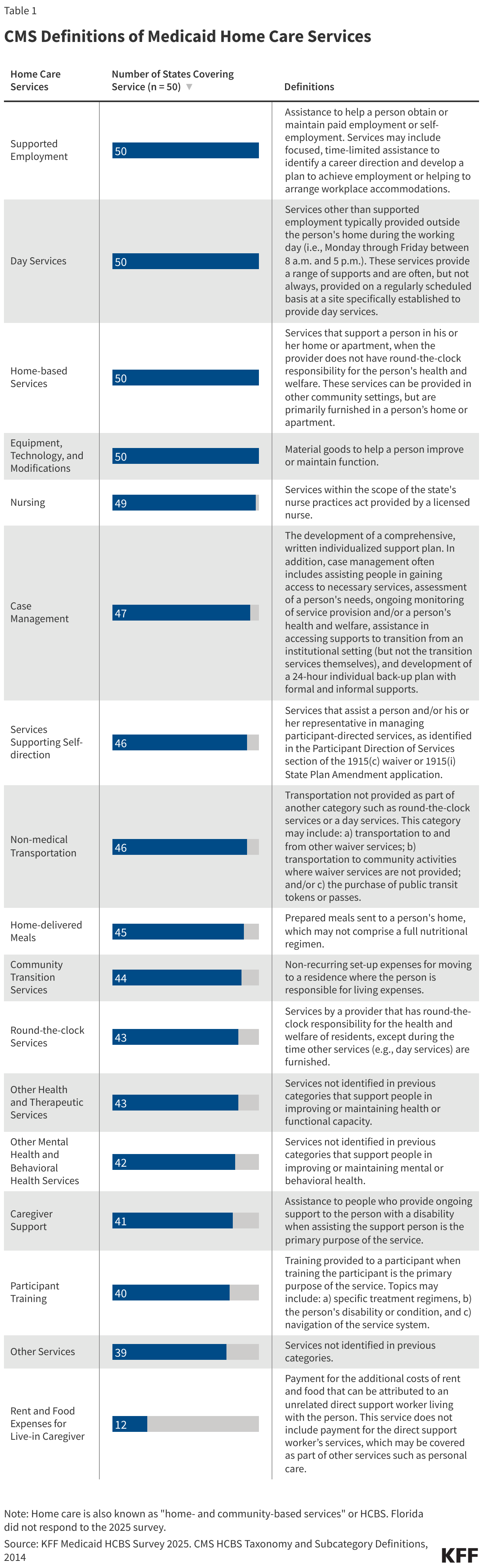
Besides personal care, Medicaid home care covers an array of services to help people with the activities of daily living and the instrumental activities of daily living. KFF asked states about what services they provide through Medicaid home care programs using the Centers for Medicare and Medicaid Services’ list of services, which are categorized in a comprehensive taxonomy. The taxonomy was developed to provide common language for describing home- and community-based services across waivers and state plans. Those services vary widely, including adult day care, supported employment, round-the-clock care, services to support unpaid family or friends who are caregivers, home-delivered meals, and non-medical transportation (Table 1).
All responding states (50) cover supported employment, day services, home-based services, and equipment, technology, and modifications in any home care program (Appendix Table 3). States often also offer other additional services for specific populations that are uniquely tailored to the needs of waiver recipients. Examples of such services reported in the 2025 survey include:
- Illness support, group counseling, and bereavement counseling in a waiver for children who are medically frail or technology dependent (Colorado);
- Discovery and career planning, additional residential supports, and community navigators in a waiver for people with intellectual or developmental disabilities (Hawaii);
- Dental services, permanent supportive housing, and prevocational/community career planning in a waiver for people with intellectual or developmental disabilities (Louisiana);
- Other speech, hearing, language, occupational, and physical therapies in a waiver for people who are ages 65 and older or have physical disabilities (Texas).
Among the categories defined by the Centers for Medicare & Medicaid Services, the least-frequently covered service was rent and food expenses for a live-in caregiver. For the most common services, there is little change in the number of states offering each type of service in a given year. (The numbers reported for most services are higher in 2025 but in many cases, that reflects a higher state response rate in 2025 than in 2024.)
States use waivers that target specific populations to offer tailored benefits, and covered services differ among different types of waivers (Figure 3, Appendix Table 4). Some services, such as equipment, technology and modifications, home-based services, and day services, are covered by most states and in most waiver programs. However, other services are much more targeted to specific populations. Comparing services among the most commonly-offered waivers (those serving people with intellectual or developmental disabilities and people who are ages 65 and older or have physical disabilities), shows some services are widely covered by one type of waiver but not the other. For example, 47 states cover supported employment for people with intellectual or developmental disabilities, but only 15 cover the service for people who are ages 65 and older or have physical disabilities, a population less likely to be working. Alternatively, home-delivered meals are covered by 41 states under waivers serving people who are ages 65 and older or have physical disabilities, but only under 10 states’ waivers serving people with intellectual or developmental disabilities. By enabling states to cover, at times, different services per target population, waivers allow states to customize services to the needs of the specific populations they serve.
Within waivers, states may change the benefit offerings from year to year, highlighting the flexibility that home care waivers offer to states in managing program benefits and spending. Focusing on the most common waivers and benefits, some notable changes between 2024 and 2025 include the following. (Due to variation in the number of states responding to KFF’s survey and changes in the number of waivers offered between 2024 and 2025, comparing the number of states or waivers offering each type of service could be misleading. However, looking at changes in covered services within a specific waiver can illuminate the flexibility available to states.)
- Oregon began offering coverage of equipment, technology, and modifications for waivers serving people who are ages 65 and older or have physical disabilities, and Idaho now covers case management services for waivers serving the same population.
- D.C. and South Dakota started offering coverage of non-medical transportation for waivers serving people with intellectual or developmental disabilities, but Illinois and Kentucky no longer cover this service for those waivers.
- Michigan, Nevada, and Washington began covering day services for waivers serving people with intellectual or developmental disabilities, and Idaho started offering this benefit for waivers serving people who are ages 65 and older or have physical disabilities.
How do states use managed care to provide home care?
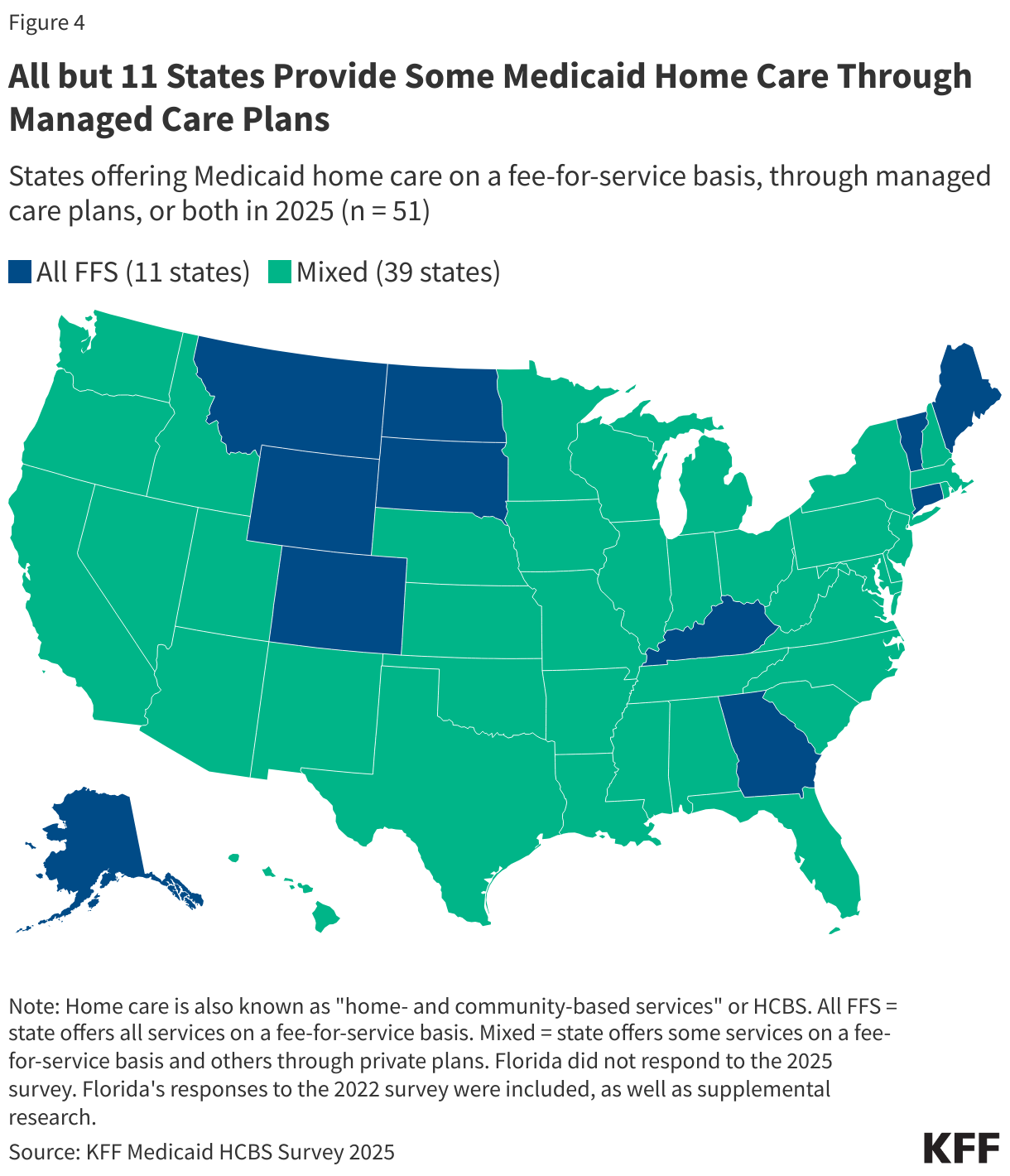
All but 11 states use managed care to provide at least some home care (Figure 4). In managed care, states pay managed care plans a set fee—often called a capitation payment—for each person enrolled and the managed care plans are responsible for providing all services to enrollees. Use of managed care to provide home care has been growing over time, with states using managed care to make their Medicaid spending more predictable and to help coordinate the services enrollees use.
Managed care is more commonly used for home health benefits provided through the state plan or 1115 waivers than for 1915(c) waivers (Figure 5, Appendix Table 5). Among the 15 states with 1115 waivers, 10 use managed care plans to provide at least some home care; and over two-thirds of states use managed care plans to provide at least some home health through the state plan. Fewer than half of states use managed care plans to provide some personal care through the state plan. For 1915(c) waivers, over half of states (26) use managed care plans, 4 more states than in 2024, but managed care was much less common for waivers serving people with intellectual or developmental disabilities—of the 47 out of 51 responding states with such waivers, only 8 provided any of the benefits through managed care.

This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.